Does Reddit.com’s r/HermanCainAward wrongfully celebrate COVID-19 deaths? To some, the subreddit is a brutal, yet necessary look at the toll of vaccine misinformation and the deaths that follow. To others, it is a cesspit of schadenfreude (taking pleasure in the pain of others) that has few, if any, redeeming qualities.
The description of the popular forum reads: “Nominees have made public declaration of their anti-mask, anti-vax, or COVID-hoax views, followed by admission to hospital for COVID. The Award is granted upon the nominee’s release from their Earthly shackles.”
An average post contains multiple screenshots of social media posts made by someone who expresses anti-vax views followed by screenshots of friends or family members reporting on the person’s sickness with COVID and, often, subsequent death. The victim’s social media posts are usually right-wing and often feature conspiracy theories as well as a set of common memes.
Outside of the nominations, one can find community support posts as well as “IPAs” or “Immunized to Prevent Award” posts, in which users report getting vaccinated after witnessing the horror presented in the forum. There are also “Redemption Awards” for those who change their minds about the vaccine, often as they are dying. (Last fall, the subreddit changed its rules to require that all names and faces of non-public figures be redacted.)
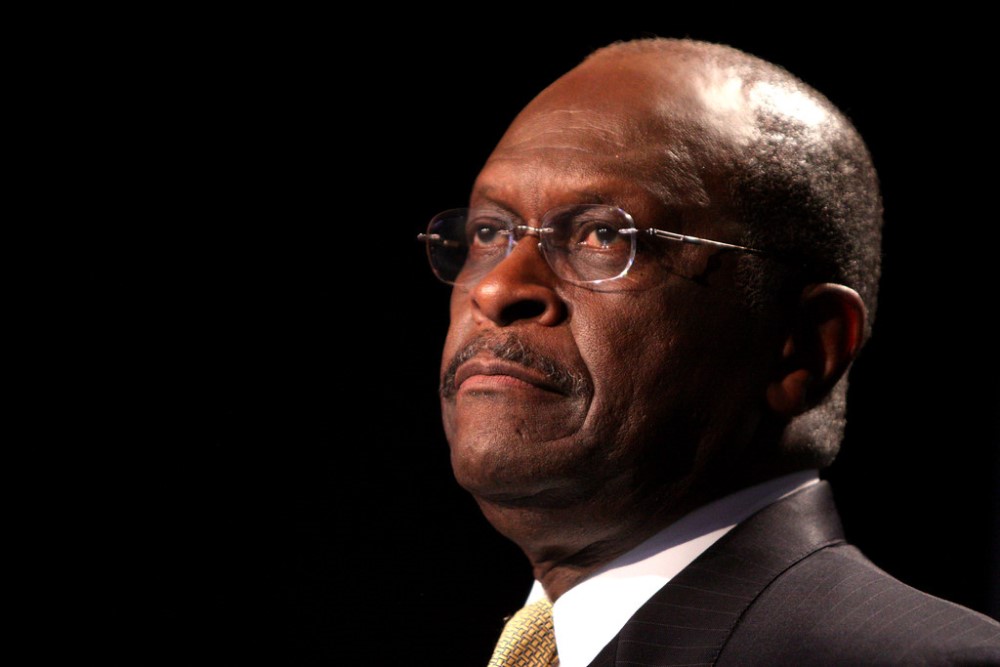
The Herman Cain Award is named after Herman Cain, a Black Republican who ran for president in 2012 and co-chaired “Black Voices for Trump” in the recent election cycle. Cain, who had prior health issues, opposed mask mandates and attended a Trump rally in Tulsa on June 20, 2020, where he was photographed not wearing a mask in a crowd of people not wearing masks. Shortly after, Cain tested positive for COVID and was hospitalized. Cain died from COVID six weeks later at 74 years of age.
To gain a better understanding of the rich, ethical dimensions the subreddit presents, there are a few questions we should ask: What is the narrative of HCA posts, and what feelings do these narratives engender? Do HCA posts, taken as a whole, accurately reflect the world around us?
Let’s start with the narratives. Perhaps the most obvious one is a narrative of righteous comeuppance. HCA nominees and winners have endangered not only themselves but also others, and they have reaped the consequences of their actions. This seems to be the primary lens of HCA viewers, who often make posts venting about the harms of anti-vax sentiments and actions.
This narrative tends to produce a sense of righteousness and stability, along with reassurance of one’s experience of the world and the moral responsibility that nominees bear. This sentiment acts as a counter to gaslighting resulting from widespread denial of the reality of the pandemic, perhaps expressed by close friends and family.
The second narrative lens appropriate for HCA content is tragedy. This is not necessarily distinct from the first lens, but it emphasizes more strongly the unnecessary suffering caused by the pandemic and our collective response to it. This lens, perhaps more than the first, encourages us to see HCA nominees as persons whose lives have value.
Pity might be too much to expect, given that the nominees are facing the consequences of their own actions, but the tragic reading does produce genuine horror at the suffering that could have been prevented. At best, this horror keeps us alive to the value of the lives lost. At worst, it devolves into a numbed-out nihilism, as we can no longer bear the burden of moral harms witnessed. It’s very easy to doom-scroll through r/HCA posts and lose hope at the possibility of change.
The third narrative is less noble than the first two. This is the narrative of the self-own — with motives that are tribal, petty, and wishing ill upon those who purport to make the pandemic worse. It is a narrative we might easily slip into from the first. This variant cares less about what is fair or appropriate and more about being right or superior. We might be especially worried about this, as the subreddit feeds off of other polarized dynamics that arise from tribal divides on the left/right spectrum. This, I believe, is the narrative that has primarily concerned those who have written against r/HermanCainAward, contending that it produces schadenfreude.
But what is troubling here is not merely pleasure in the pain of others but something stronger: pleasure in the death of others (and if not death, then extreme physical distress). Is it ever permissible to take pleasure in the death or pain of others? It seems acceptable to take comfort in knowing someone can no longer do any harm, but a preventable death is a bad thing that we should never see as good.
If we take pleasure in the deaths of others, we must either take up some view on which their death is deserved and proportional to their crimes or else discount the value of that person’s life. Neither is an attractive option. Even if nominees have caused the deaths of others by spreading the virus, it is a strong view to claim that their own deaths are deserved because of their actions. And assuming that their deaths were deserved, it still might seem unsavory to take pleasure in their punishment. But the predominant kind of gratification appears to fall into the category of feeling somehow superior to those who are dying. Self-satisfaction at the downfall of others is rather ugly.
These critiques do not rule out righteous anger or the recognition that r/HCA nominees have flouted moral requirements. But they do require that we not reduce them to faceless, nameless monsters that lose their humanity when relegated to a series of memes. The Reddit.com rule changes actively made this aspect worse, even if they helped to prevent doxing.
Does r/HCA currently represent the reality of vaccine denial? The answer seems to be no. The posts that receive attention on r/HCA are for those who are hospitalized and sometimes die from the virus, but there are other unvaccinated individuals who have relatively mundane experiences of the virus. Yes, the unvaccinated are significantly more likely to die, but r/HCA displays the same kind of data skewing as the programming on The Weather Channel — the most extreme cases are given the most attention.
Is there some version of r/HCA that could preserve its prosocial functions and avoid its morally problematic elements? Perhaps, but it would look drastically different from the current subreddit. First, the subreddit would need to include more representative individual stories that capture the variety of experiences of those living through a pandemic. Second, the people featured would need to be more humanized, with more details about their lives included beyond their online, meme-sharing activities. Third, the community should be reworked so it is not constructed in an us-vs.-them dichotomy, where pro-vaxxers are unequivocally the good guys and anti-vaxxers are unequivocally the bad guys.
Would the subreddit be as popular if it were reconstructed in that way? Probably not. But we might start to see each other as human again.